


_and_hallux_valgus.tiff)
Introduction
The characterization and classification of first metatarsal regeneration (FMR) after new modern minimally invasive bunion surgery (MIBS) has yet to be described. Recently, minimally invasive (MI) bunion surgery has seen a tremendous resurgence due to improved techniques, and advances in surgical hardware and instrumentation.1–8 While several methods for MIBS have been described, subcapital metatarsal realignment osteotomy with percutaneous MI bone screw fixation appears to be widely popular.1,9–20 The technique calls for extreme shifts in metatarsal head position where there may be little to no bone apposition (or contact) with the proximal metatarsal shaft,9–12 raising questions/concerns as to whether or not the bone will heal. Unlike traditional osteotomy bunion surgery with screw fixation, MIBS bone healing occurs through secondary bone healing (callus formation) with the goal of complete “first metatarsal bone regeneration” (a new term we are coining) in a new realigned remodeled corrected position. The regenerative process with MIBS is poorly understood and has yet to be studied or classified, and the goal of this investigation is to define the patterns of healing/FMR.
Methods
The authors conducted a retrospective review of the senior authors (N.M.B.), first and consecutive cases of patients who had undergone MIBS from January 2018 to June 2021. Medical databases, charts, and radiographs were reviewed. To be included in the cohort required having undergone MIBS without other osseous procedures of the first ray. Patients who underwent MIBS in conjunction with other procedures that did not permit immediate postoperative weightbearing were excluded. A minimum of four months of follow-up was required to be included, as we determined this timeframe to be the minimal amount of time where bone callus would be sufficiently present on radiograph. Also excluded were patients where bone healing could not be assessed due to: lost to follow-up (unavailable radiographs), had previous bunion surgery involving osteotomy and/or first ray fusion surgery of any kind, and/or postoperative complications (involving infection requiring incision & drainage, fixation failure and/or postoperative metatarsal fracture/explosion, and/or requiring additional surgery prior to healing). The following data was collected: age, sex, laterality and postoperative weightbearing device.
Radiographic angles and number of metatarsal screws were obtained. Radiographic assessments and measurements were performed with a digital imaging system (20/20 Imaging, Konica Minolta Americas, Inc., Crystal Lake, IL). Standard radiographic weightbearing views anteroposterior and lateral views were obtained. A single measurement was taken for each radiographic variable (angular measurement and FMR) by a single junior author. Successful radiographic healing was determined using the following criteria on 2 more radiographic views: callus formation and/or trabeculation around/at the osteotomy with no evidence of sclerosis, with no broken or loose hardware.
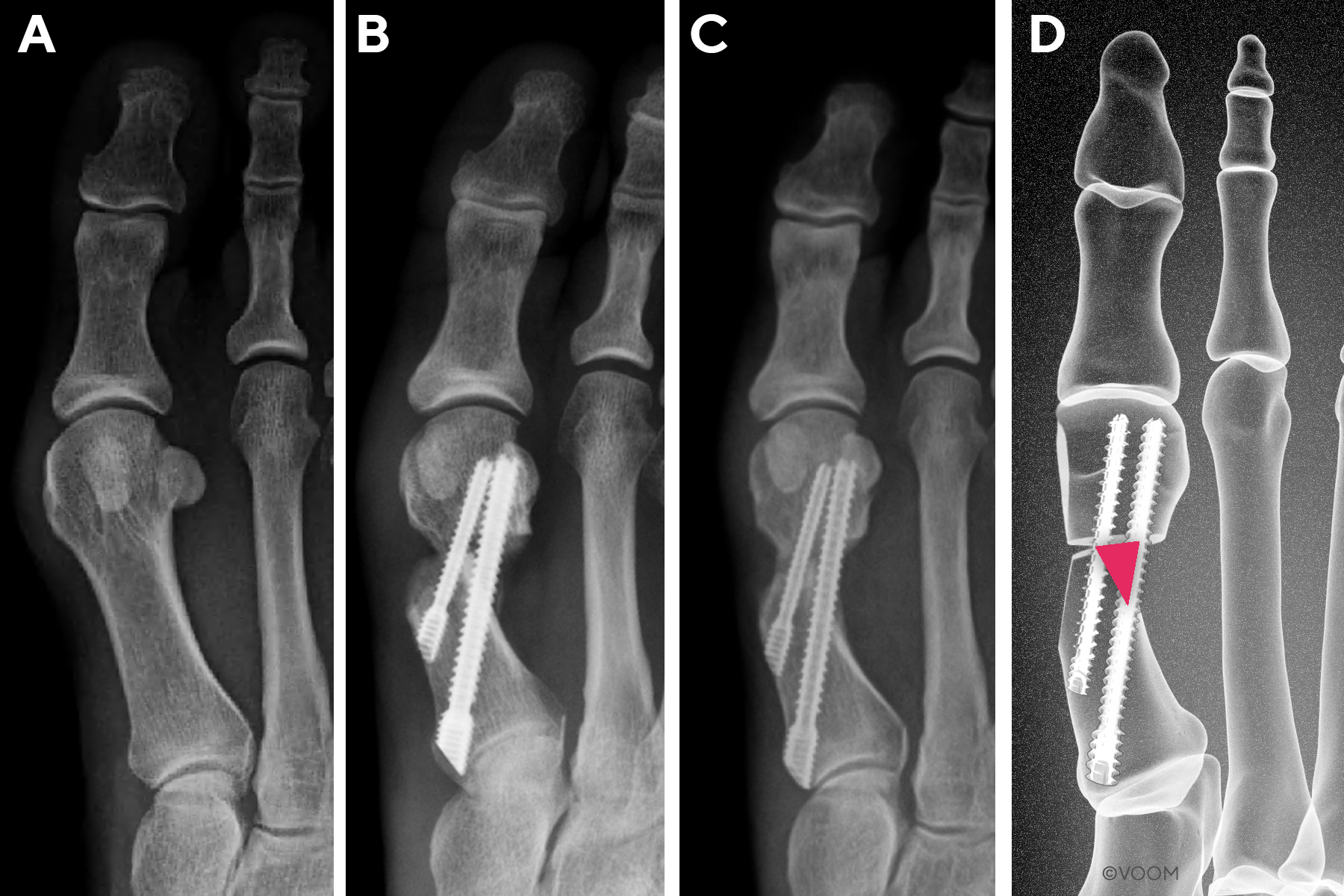
The area where bone healing occurs with new MIBS is located in a triangular zone lateral to the first metatarsal shaft and proximal to the subcapital osteotomy, which we herein define (and coin) as the regeneration triangle (Figure 1). Distinct patterns of metatarsal healing and regeneration may occur in this regeneration triangle. We classified them into our newly developed FMR classification system with three types (FMR Types I, II, III) (Table 1 & Figures 2-4), based on bone healing in relation to the MI anchor bone screw. The “anchor” screw is the dominant screw in the fixation construct of a new MIBS that connects the proximal metatarsal segment to the translated metatarsal head.22 Radiographic bone healing assessments were reviewed and graded, based on the anteroposterior radiograph; however, additional views were assessed to verify union when necessary.

_type_i.jpg)
_type_ii.jpg)
_type_iii.jpg)
New First Metatarsal Regeneration Classification System (Figures 2-4)
First Metatarsal Regeneration Type I: Callus formation located only medial to the MI anchor bone screw (Figure 2).
First Metatarsal Regeneration Type II: Callus formation located medial and lateral to the MI anchor bone screw (Figure 3).
First Metatarsal Regeneration Type III: Robust callus formation with first metatarsal regeneration (Figure 4).
The statistical analyses were performed using Statistica® 13.1, and a two-sided P < 0.05 was considered significant in all analyses. Continuous variables were reported as mean ± standard deviation (SD) with 95% Confidence Interval (CI). Categorical variables were reported as numbers and percentages. Comparisons between FMR groups were performed using a T-test, U-Mann–Whitney test, Kruskal-Wallis ANOVA, Wilcoxon matched pairs test, and chi-square, as appropriate. The correlation analysis was performed with Pearson or Spearman-rank test, as appropriate.
Surgical Procedure
All patients underwent a minimally invasive subcapital metatarsal realignment osteotomy with percutaneous screw fixation using modified third generation minimally invasive approach.9–12 This involved a subcapital realignment of the distal aspect of the first metatarsal osteotomy using a Shannon bur combined with percutaneous first generation MI bone screw fixation by placing 1 to 2 screws across the osteotomy site.9–12,21,23 Anesthesia was either general or monitored anesthesia care along with an ankle block using local anesthetic. Cases were performed without a tourniquet. Intraoperative fluoroscopic imaging with a mini C-arm was used in all cases. The method and technique was modified (over time) for some patients using proprietary methods of the senior author.
Osseous and joint landmarks are identified and marked with the use of intraoperative fluoroscopy.9–12,23 Two skin incisions were created. The first incision was made at the medial neck of the first metatarsal. A second incision was made at the medial base of the first tarsometatarsal joint. Dissection of these incisions were bluntly performed to gain access to the bone.
Attention was first directed at the distal incision where a periosteal elevator is used to create a plane between the bone of the first metatarsal neck and dorsal soft tissue structures. The subcapital osteotomy is performed with a rotary 2.0 mm shannon burr under fluoroscopic guidance and irrigation. A through-and-through extra-capsular subcapital osteotomy was made from medial to lateral and dorsal to plantar.9–12 Either a transverse, modified chevron/chevron type, or proprietary Transveron™ osteotomy was performed depending on surgeons clinical preference.23 Most commonly, a Transveron™ osteotomy was performed.23
The lateral translation of the first metatarsal head was performed with an elevator or hemostat placed into the proximal metatarsal shaft, using the diaphyseal cortex as fulcrum for translation. The metatarsal head was laterally translated to reduce intermetatarsal angle, and the head rotated to restore the frontal plane position of the sesamoids.9–12,23
Fixation of the metatarsal head was achieved by placing a first generation MI bone screw through the proximal incision. Minimally Invasive Chevron Akin screw fixation (Stryker Corp, Kalamazoo, MI) was used. The screw(s) was placed over a guidewire, which was placed using fluoroscopic assistance. In all cases, a 4.0 mm screw was placed obliquely within the first metatarsal, originating from the flare of the medial base of the first metatarsal into the capital fragment, while engaging the lateral diaphyseal cortex of the first metatarsal. In some cases, an additional point of fixation was placed using an additional 4.0 mm screw or a 3.0 mm screw just distal and parallel to the first screw. This screw was either placed through the same proximal incision or through an ancillary percutaneous incision, also using intraoperative fluoroscopic assistance.
The overhanging redundant bone shelf of the proximal medial metatarsal shaft was resected with a burr. The bone fragment(s) were either removed or pushed into the metatarsal canal as bone graft. A percutaneous adductor release was performed if needed using a beaver blade under fluoroscopic guidance.2,23,24 An Akin osteotomy was additionally performed if clinically necessary.
Postop Protocol
The postoperative protocol involved immediate full weightbearing as tolerated in a postoperative surgical shoe regardless if unilateral or bilateral surgery was performed. A cane was dispensed for all patients to use as tolerated, if needed. We did not measure or keep any record of the actual amount of weight applied to the operated foot/feet during the postoperative period and/or the number of steps taken. At around 6 weeks, patients transitioned into a stable sneaker.
Results
The results are tabulated in Table 2. A total of 172 feet in 122 patients fulfilled the inclusion criteria. Five patients (4.1%) were male and 117 (95.9%) were female. The mean age of the patients at the time of surgery was 46.6±14.6 years (95% CI, 44.5–48.9 years). The FMR staging was as follows (n=172): 30 feet (17.4%) achieved Type I FMR, 73 feet (42.4%) achieved Type II FMR healing and 69 (40.1%) Type III achieved FMR (Table 3). There was a statistically significant overall difference in IM and HVA before and after the procedure (p<0.001 and p<0.001, respectively) (Table 4, Figure 5). This statistically significant pre- and post-operative angle difference was maintained across all FMR types (I-III, p<0.001 for all comparisons). We performed a correlation analysis between the FMR type, baseline characteristics, and procedural information (age, sex, laterality, operation on both or one feet, length of follow-up, pre-operative and post-operative angles, and number of screws used). There was no statistically significant correlation.
_and_hallux_valgus.tiff)
A total of 50/122 (41%) patients were operated on both legs, and among those, 24/50 (48%) were operated on the same day. Overall, 12/50 (24%) of patients operated on both legs had the same FMR type on both feet when the procedure was done on the same day and 10/50 (20%) when the procedure was performed on a different day. Difference between FMR types was seen in 14/50 (28%) of people between the legs for both same and different day surgery groups. This difference is not statistically significant (p=0.389). Details are summarized in Table 5.
Discussion
Due to the ‘newness of MIBS’ and the perceived uncertainty of osseous healing with an unconventional fixation method, it is important and necessary to classify the extent of FMR after new MIBS as this technique becomes more accepted and widespread. No prior study has attempted to standardize or stratify metatarsal regeneration objectively, either with plain film radiographs or with CT, especially in a large cohort of patients who underwent MIBS. Proponents and early adopters of MIBS have clinically witnessed metatarsal healing using these techniques with extreme metatarsal shifts; however, were lacking significant research studies to confidently corroborate this healing. This retrospective study not only demonstrates bone healing potential but also the propensity for complete metatarsal regeneration.
We chose to use the hardware as the delineation line between the medial regeneration triangle (FMR Type I) with some bone-to-bone contact versus the lateral regeneration triangle (FMR Types II & III) where there would likely be significant separation between the bony segments. In a frequent fixation construct, the hardware (MI anchor bone screw) is generally located centrally in the metatarsal head and this delineation line generally splits the regeneration triangle in half. The benefit of differentiating between the medial healing from lateral healing distinguishes the medial zone which would have more bone-to-bone apposition whereas the lateral zone would have less, if any, bone-to-bone apposition. In essence, the medial healing would be considered ‘easier’ healing versus the ‘harder’ lateral healing where much more bone deposition/callus formation might be required. Additionally, the smaller metatarsal translations would have a smaller area regeneration triangle and conversely a larger metatarsal translation would have a regeneration triangle with a larger area.
Hardware position, number of screws and extent of metatarsal shifting influenced how we distinguished between FMR Type II versus FMR Type III. Fortunately, the fixation construct is generally consistent with the anchor screw being placed centrally in the metatarsal head. In situations where extreme metatarsal head shifts and/or laterally placed hardware (in the metatarsal head) increases the medial regeneration triangle and shrink the lateral regeneration triangle, effectively converting a FMR Type III to FMR Type II. This scenario also occurs when two screws were used as it might allow for more available space for healing with complete metatarsal regeneration. Nonetheless, there are situations where there is Type II healing, but not complete metatarsal regeneration, therefore there is merit in keeping the FMR Type III complete metatarsal regeneration as a distinct category. As such, a FMR Type III signifies robust metatarsal regeneration.
The clinical significance of more or less bone healing (FMR Type) was not the focus of this investigation, rather our goal was to identify patterns of healing in this new MIBS. All three FMR types constitute healing and are considered a satisfactory healed outcome. The majority of the feet (n=142, 82.5%) healed with more extensive lateral bone regrowth (Type II & III). It is presumed that FMR Type III complete metatarsal regeneration is a more optimal result because the first metatarsal surface area would be greater in this healing zone. Conversely, a FMR Type I could potentially be a more fragile result leading to future issues such as stress fracture. Our clinical experience (not studied here) finds no difference between FMR type and patients satisfaction/outcomes. However, there is no evidence to support any of these notions based on this study, and is indeed an area for future investigation.
This study demonstrated that bone healing and regeneration occur with this unconventional first ray realignment technique where the metatarsal head is significantly displaced from its shaft, in a clinical model involving MI bone screw fixation utilizing single or dual metatarsal screws. The majority of our cases (85%) involved a single MI anchor bone screw for fixation (n=147) and there was no statistically significance in healing with a double metatarsal MI bone screw construct (n=25,14.5%). However, our sample size of a two MI bone screw fixation construct was small in this retrospective study, which is likely why statistical relevance could not be achieved.
The ideal fixation construct has yet to be established and two screw fixation has been classically promoted. In contrast, our preferred method for MIBS is a single screw fixation. We recognize that traditional fixation constructs for osteotomy and bone fusion often require rigid fixation in multiple planes. However, MIBS surgery involves large bony shifts with little to no bone contact where the fixation instead acts as a metallic scaffold for bone regeneration. As such, the classic principles for multiplanar rigid fixation do not particularly apply here, and this study demonstrates the ability of bones to heal/regenerate with single screw MIBS fixation. Furthermore, since a single MI anchor bone screw might be radiographically perceived as a less stable construct and that healing can occur even with weight-bearing indicates that single MI bone screw fixation is indeed adequate fixation to support both healing and weight bearing. Future studies that clinically compare single versus dual metatarsal screw fixation are the next logical studies to emerge with MIBS.
This retrospective study only reviewed a fixation construct that involved first generation MI bone screws. The features of an MI bone screw are: 1) a beveled head to allow the screw to lay flush with the bone, 2) threaded head to capture bone at the insertion site, 3) a fully-threaded shaft with a cortical pitch to optimally purchase the lateral first metatarsal cortex, and 4) non-compressive and neutral pitch between head and shaft.12 The technique for new MIBS calls for a MI bone screw as it provides bone engagement/stability between the head, lateral metatarsal shaft and the metatarsal base. The FMR ability of other kinds of screws, plates and/or fixation constructs are unknown and also an area of future investigations, especially as a comparison to this benchmark MI bone screw study.
Surgical technique and experience evolved over time which might have influenced the results of this study. It is well known that a learning curve exists with MIBS and cases early in this retrospective review might have resulted in less precise actions, leading to altered healing.25–28 Nuances and techniques did indeed evolve during the 3 year span of this study, involving an even less traumatic proprietary method to the soft tissues and bones. Studies that evaluate less disruptive and invasive measures to the soft tissues on bone healing will likely be another area where research emerges. Osteotomy configuration and location may also impact bone healing based on the surface area of exposed osteotomized bone.
The purpose of this study was to characterize and classify the regenerate bone that occurs after MIBS, and only retrospectively reviewed patients who went onto radiographic healing. By design we excluded patients who had complications that would have interfered with the bone healing process or developed symptomatic nonunion. We did not study the rate of union with MIBS and is an area for future investigation, particularly with a walking recovery. Because all of the patients were allowed immediate full weight bearing as tolerated in a postop shoe, it is unknown if weightbearing affected the healing potential or metatarsal regeneration capability positively or negatively. Since weightbearing is a more desirable postoperative protocol after bunion surgery, these results, at the minimum provide evidence that adequate bone healing does indeed occur with a walking recovery in postoperative shoe with MIBS where extreme shifts in metatarsal head position can occur (in other words, for bunions of all severities). In addition, these results also provide a healing type stratification and benchmark for which to compare future studies that look to classify healing potential and various weightbearing protocols, whether they be more restrictive or more aggressive.
This study indicates that there appears to be no statistically predictability on FMR type from one foot to the other when patients had bilateral MIBS, on the same day or different days. A large number of patients in this study had MIBS on both feet, accounting for 41% of the cohort, with nearly half (48%) of them having same day bilateral MIBS. Whether patients had unilateral MIBS or bilateral MIBS (same day or different days) did not affect FMR type. Interestingly, and not statistically significant, there is an observation that the same healing FMR type occurs between feet (28% for same day and 20% for different days). Again, it must be pointed out that we did not study union rate and cannot answer the statistical question of healing rate between feet, but bilateral FMR predictability is an interesting data point that resulted from this study when patients radiographically healed.
While MIBS demonstrated a statistically significant correction of IMA and HVA (which was maintained for all FMR types), there was no significant correlation to FMR types. Being that we operated on bunions of all severities with the mean preoperative IMA of 15.8° (smallest being 12.1° and the largest being 19.5°) indicates this study examined the total range of bunion severity healing. One would postulate that more robust healing would occur with larger bunions with a theoretically larger regeneration triangle, but this was just not the case. This study suggests that bunion severity and its angular correction might be an irrelevant factor for healing propensity, and an area for further investigation that also incorporates union rate.
Our investigation was focused on the radiographic characteristics of FMR and did not correlate bone callus with age, gender, or medical comorbidities. Not surprisingly our bunion population consisted mainly of women who represented 95.9% of the cohort. Perhaps these variables could affect the amount of callus deposition or FMR distribution with MIBS and an interesting area for focused investigation.
This study is limited as it’s a retrospective analysis simply looking at the radiographic ability of the first metatarsal regenerate after MIBS. We did not study or analyze patient medical comorbidities, weight, habits (i.e., smoking) which would all be useful data points to correlate. Our study eliminated patients with complications (such as infection, repeat surgery for malunion/nonunion) and would be an area of future investigation to assess FMR when complications do occur. Perhaps a longer follow up study than we provided (8.2±5.7 months) might yield different FMR staging percentages, particularly for Type I as additional healing might occur at a later date. Being that this was a single surgeon (N.M.B.) consecutive series beginning with first cases, surgeon variable bias did not occur which might have impacted the outcomes in either direction. While there are dozens of methods for MIBS, the surgical technique and screw construct had evolved over time and this was not accounted for. Additionally, different surgeons/techniques may have completely different FMR profiles. Multicenter comparative studies would be valuable to compare different MIBS methods/techniques/constructs. Importantly, this is a radiographic retrospective study to demonstrate healing patterns and not any possible clinical outcomes or symptomatology associated with FMR and indeed the next important study needed. This current retrospective study’s goal was to provide evidence and characterization of adequate bone healing after MIBS in a large series of patients, and will undoubtedly provide a framework for future targeted investigations on variables we did not study.
Conclusion
First metatarsal regeneration is a new phenomenon that occurs as a result of modern percutaneous realignment distal first metatarsal osteotomy with screw fixation. The paucity of literature/evidence on how/if the first metatarsal heals has created surgeon hesitancy on learning/implementing these bunion repair techniques.
This investigation presents a new and novel radiographic classification system for FMR after MIBS. This study not only addresses the question “if the first metatarsal bone can heal” but particularly demonstrates a framework on “how the bone will heal.” It’s the first study to provide radiographic patterns of healing (three distinct types) of first metatarsal bone regeneration after MIBS for all bunion severities with an immediate walking recovery in a surgical shoe. Surgeons considering adding MIBS to their bunion treatment armamentarium should no longer fear that bone healing is not possible. Our classification will help guide future studies by assisting in comparing the healing potentials of different techniques, fixation types/constructs and weight bearing protocols.
Disclosure Statement
Neal M. Blitz DPM is the CEO of Voom Medical Devices, Inc and receives compensation for this role. David T. Wong reported no disclosures. Bogdan Grecea DPM is the Director of Surgeon Onboarding for Voom Medical Devices, Inc and receives compensation for this role. Eric S. Baskin DPM is the Director Surgeon Training for Voom Medical Devices, Inc and receives compensation for this role.
Financial Declaration
The authors received no financial support for the research, authorship, and/or publication of this article. Artistic drawings/renders provided by Voom Medical Devices, Inc.
Funding
None
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
Corresponding Author
Neal M. Blitz, DPM
Email: nealblitz@gmail.com