



Introduction
New minimally invasive (MI) bunion surgery has become increasingly popular in recent years due to advances in techniques and surgical implants.1–10 This method has created a host of new and serious complications that didn’t exist with traditional bunion surgery. Metatarsal explosion is an uncommon complication that has yet to be reported, studied and classified.
This investigation presents a radiographic classification system for metatarsal explosions, proposed mechanism of occurrence and provides a treatment paradigm. Better understanding of these types of metatarsal fractures associated with new minimally invasive bunion surgery (MIBS) will help surgeons manage and avoid these complications in the first place.
Methods
The authors conducted a retrospective review of each of the authors cases to identify patients who had a metatarsal explosion after minimally invasive subcapital metatarsal realignment osteotomy with percutaneous screw fixation from January 2018 to May 2022. Medical databases, charts, and radiographs were reviewed. Inclusion in the cohort required having undergone MIBS with any forefoot procedures, so long as it allowed for immediate postoperative weight bearing. The following data was collected: age, sex, medical history, BMI and postoperative weight bearing device.
Radiographic angles, number of screws and positional measurements were obtained. Radiographic assessments and measurements were performed with a digital imaging system. Standard radiographic weightbearing views anteroposterior and lateral views were obtained for preoperative angular measurements, and postoperative metatarsal explosion radiographs may have been non-weight bearing films. A single measurement was taken for each radiographic variable.
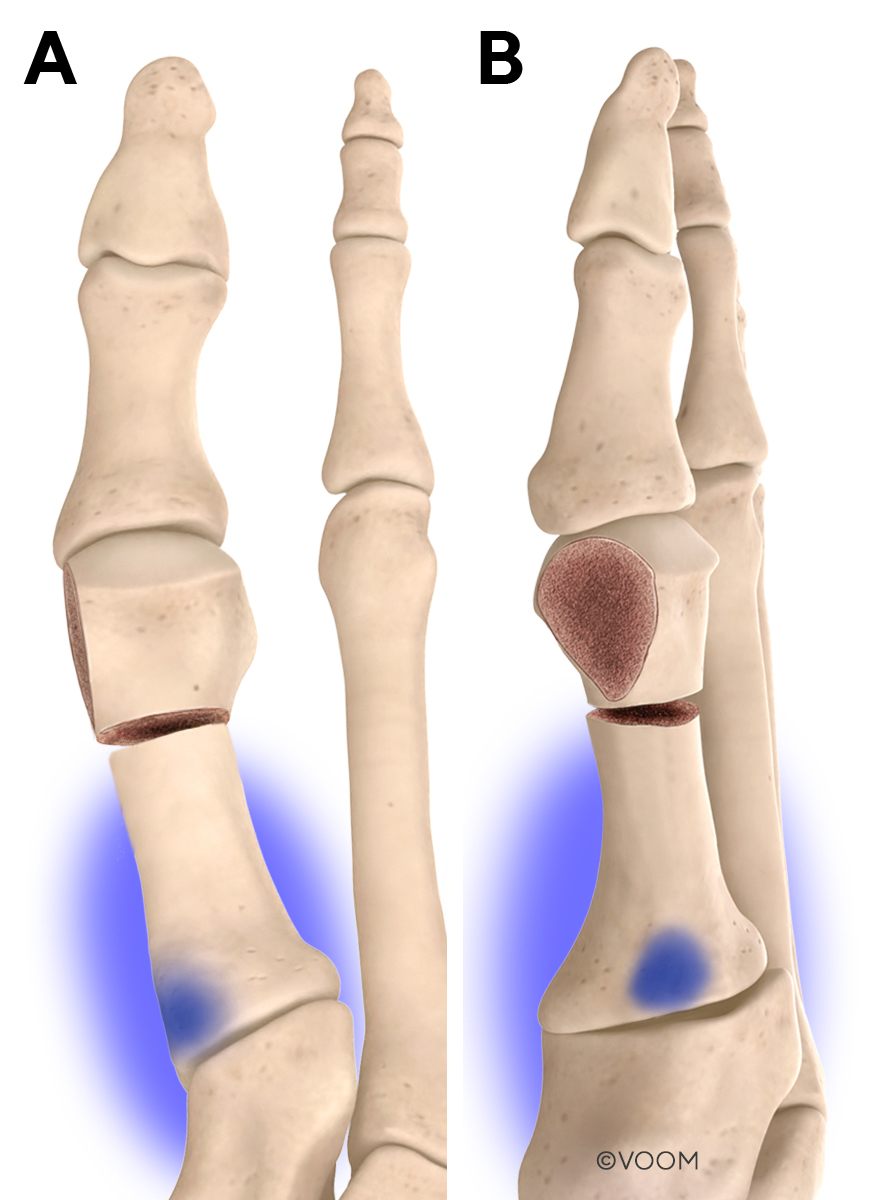
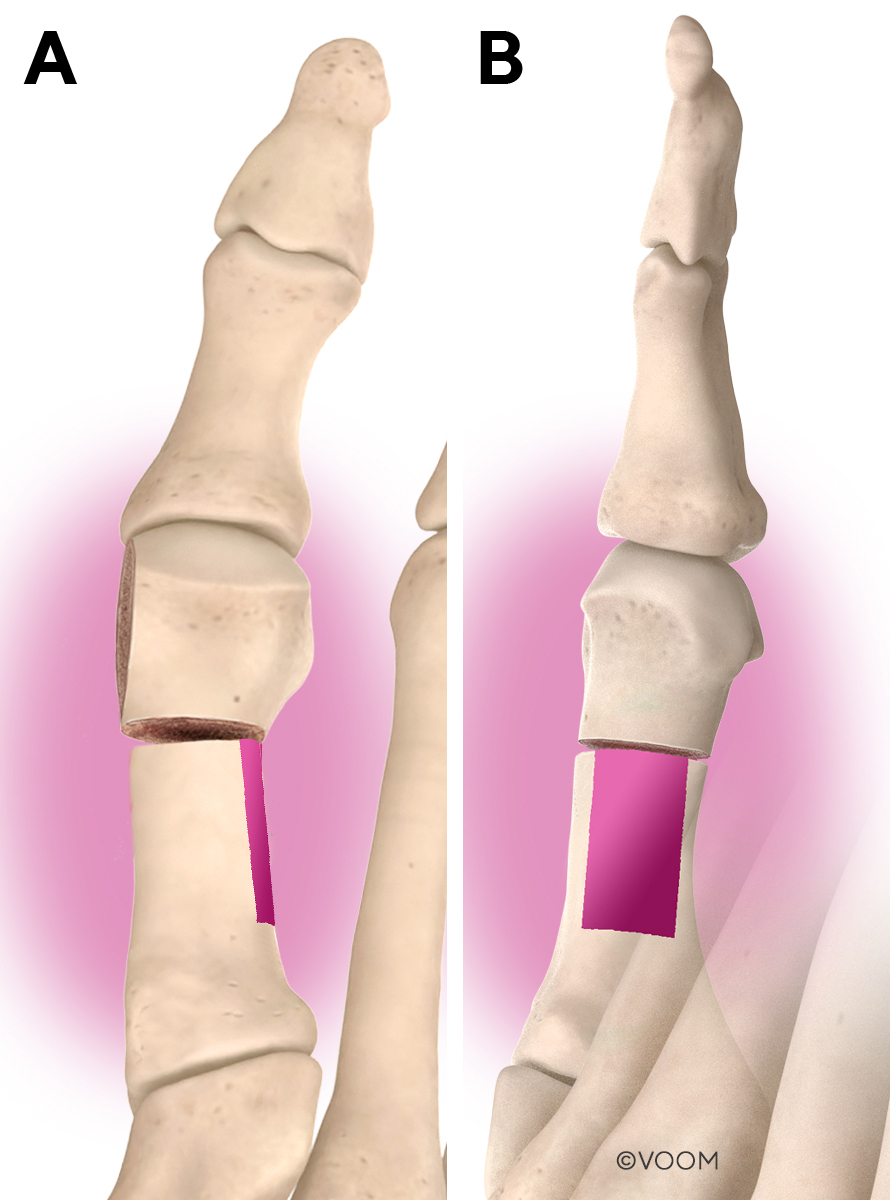
We also evaluated the locations of the MI screw(s) entry point within the metatarsal base and exit point at the lateral metatarsal shaft. The entry zone in the medial metatarsal base, we coin the term “Cancellous Anchor Zone” (CAZ) (Figure 1). The exit zone in the distal lateral metatarsal shaft, we coin the term “Cortical Purchase Zone” (CPZ) (Figure 2). Screw(s) within the CPZ found to be in close proximity to the osteotomy were identified as a possible etiologic cause of metatarsal explosion. Screw(s) in the CAZ that were dorsal and/or distal were also identified as a possible etiologic cause of metatarsal explosion.
Radiographic assessments were reviewed and graded in each foot with the newly developed metatarsal explosion classification system (see Table 1 & Figure 3) that identifies the fracture pattern along with a pathognomonic radiographic finding. Metatarsal explosion type was based on various radiographic views, and CT scans were used when available.
.jpg)
.jpg)
.jpg)
The statistical analysis was conducted using Stata MP/17 for macOS. Qualitative data were expressed as frequencies and percentages, while quantitative variables were expressed as median and interquartile range (IQR). Mann-Whitney test was used to compare the association between metatarsal explosion type, screw number, and comorbidities with continuous variables. Pearson’s Chi-squared test, with Fisher exact when needed, was used to compare categorical variables. All tests were two-sided. Statistical significance was set at a p-value <0.5.
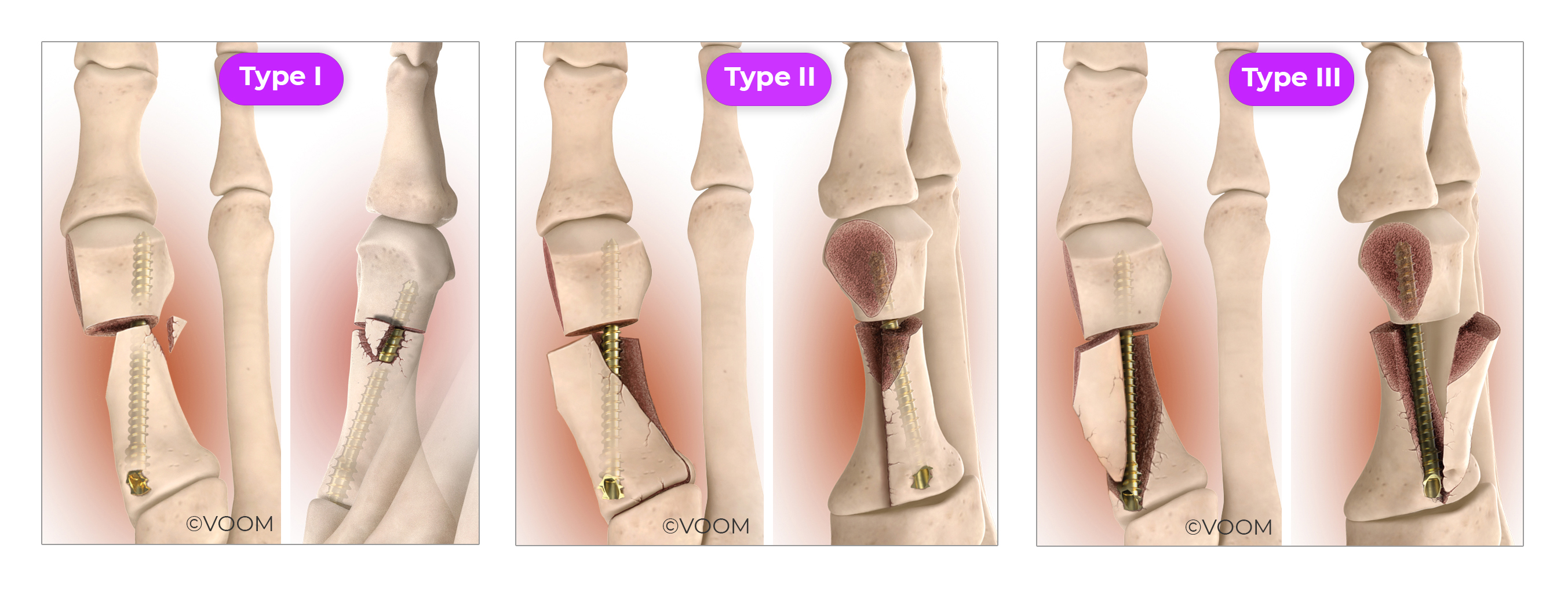
New Metatarsal Explosion Classification System (Figures 3 & 4)
Metatarsal Explosion Type I: A distal lateral metatarsal shaft fracture between the metatarsal osteotomy and MI bone screw(s) exit point at the CPZ. The radiographic features are fleck fracture(s) at the screw-bone interface.

Metatarsal Explosion Type II: Complete through-and-through transverse plane fracture of the metatarsal shaft and base that starts at the MI bone screw(s) exit point at the CPZ and extends proximally into the tarsometatarsal joint (intra-articular). The hallmark radiographic feature, we herein coin, the “double metatarsal sign”.
Metatarsal Explosion Type III: Multiple fractures of the metatarsal shaft and base also starting at the MI bone screw(s) exit point at the CPZ and travels along the plane of the fixation, ending extra-articular to the first tarsometatarsal joint, and invading the CAZ. The resultant dorsal butterfly fragment is the hallmark radiographic feature.
Surgical Procedure
All patients underwent a minimally invasive subcapital metatarsal realignment osteotomy with percutaneous screw fixation using modified third generation minimally invasive approach.1,11–14 This involves a subcapital realignment first metatarsal osteotomy using a Shannon bur combined with percutaneous first generation MI bone screw fixation by placing 1 to 2 screws across the osteotomy site.1,11–14 Anesthesia was either general or monitored anesthesia care along with an ankle block using Lidocaine. Cases were performed with and without a tourniquet based on surgeon preference. Intraoperative fluoroscopic imaging with a mini C-arm was used in all cases. The method and technique was somewhat different between surgeons based on their expertise.
Osseous and joint landmarks are identified and marked with the use of the mini C-arm.1,11–14 Two skin incisions were created. The first incision was made at the medial neck of the first metatarsal. A second incision was made at the medial base of the first tarsometatarsal joint. Dissection of these incisions were bluntly performed to gain access to the bone.
Attention was first directed at the distal incision where a periosteal elevator is used to create a plane between the bone of the first metatarsal neck and dorsal soft tissue structures. The subcapital osteotomy is performed with a rotary 2.0 mm shannon burr under fluoroscopic guidance and irrigation. A through-and-through extra-capsular subcapital osteotomy was made from medial to lateral and dorsal to plantar. A through-and-through extra-capsular osteotomy was made from medial to lateral and dorsal to plantar.1,11–14 Either a transverse, modified chevron/chevron type, or proprietary Transveron™ osteotomy was performed depending on surgeons clinical preference.14
The lateral translation of the first metatarsal head was performed with an elevator or hemostat placed into the proximal metatarsal shaft, using the diaphyseal cortex as fulcrum for translation. The metatarsal head was laterally translated to reduce intermetatarsal angle, and the head rotated to restore the frontal plane position of the sesamoids.1,11–14
Fixation of the metatarsal head was achieved by placing a first generation MI bone screw through the proximal incision. Either Minimally Invasive Chevron Akin screw fixation (Stryker Corp, Kalamazoo, MI) or Arthrex screw fixation (Arthrex Inc, Naples, FL) was used. The screw was placed over a guidewire, which was placed using fluoroscopic assistance. In all cases, a 4.0 mm screw was placed obliquely within the first metatarsal, originating from the flare of the medial base of the first metatarsal into the capital fragment, while engaging the lateral diaphyseal cortex of the first metatarsal. In some cases, an additional point of fixation was placed using an additional 4.0 mm screw or a 3.0 mm screw just distal and parallel to the first screw. This screw was either placed through the same proximal incision or through an ancillary percutaneous incision, also using intraoperative fluoroscopic assistance.
The overhanging redundant bone shelf of the proximal medial metatarsal shaft was resected with a burr. The bone fragment(s) were either removed with a hemostat or pushed into the metatarsal canal as bone graft. A percutaneous adductor release was performed if needed using a beaver blade under fluoroscopic guidance.1,11–14
Postop Protocol
The postoperative protocol involved immediate full weightbearing as tolerated in a postoperative surgical shoe regardless of a unilateral or bilateral surgery performed unless the patient had an existing comorbidity where a CAM walker was issued based on surgeon preference. A cane or crutches was dispensed for all patients to use as tolerated, if needed. We did not measure or keep any record of the actual amount of weight applied to the operated foot during the postoperative period and/or the number of steps taken. Our protocol is to transition patients into a stable sneaker at around 6 weeks, but given the nature of this retrospective study patients had metatarsal explosions precluding them from the standard transition protocol.
Results
The demographic data is provided in Table 2. The description of patients’ data is provided in Table 3. Sixteen feet (15 patients) were included in the present study. The median age of the included patients at the time of surgery was 61.6 (52 to 76) years, and 80% of the patients were females. The median body mass index (BMI) of the included patients was 28.2 (22.9 – 39.5) Kg/m2, and 40% of the patients were obese (BMI > 30 Kg/m2). Forty percent of the cases had thyroid disorders. Nearly two-thirds of the metatarsal explosion cases were on the left side. One patient had a bilateral metatarsal explosion. Treatment was non-surgical with protected partial weight-bearing (PPWB) for 12 feet (75%) and surgery open reduction internal fixation (ORIF) for 4 feet (25%).
The metatarsal explosion staging was as follows (n=16): 8 feet (50.0%) with Type I metatarsal explosion, 5 feet (31.25%) with Type II metatarsal explosion and 3 feet (18.75%) with Type III metatarsal explosion (Table 4).
The etiologic association of screw placement with metatarsal type is listed in Table 5. For this analysis, we distinguished between distal fractures (Type I) and those that also progress proximally (Type II & III). Twelve feet (75.0%) of all metatarsal explosions had screw(s) distal in the CPZ, and 7 feet (43%) of all metatarsal explosions had screws distal and/or dorsal in the CAZ. The association analysis showed no overall association between the etiologic association of screw placement and metatarsal type (p =0.66). Likewise, the distribution of metatarsal type was not different in patients with screws distal in CPZ (p =0.683) and those with screws distal and/or dorsal in the CAZ (p =0.653).
The association between the metatarsal explosion type and other parameters are listed in Table 6. The distribution of metatarsal explosion types was not significantly associated with age (p =0.67), gender (p =0.43), laterality (p =0.41), BMI (p =0.09), preoperative IM (p =0.37), and all medical comorbidities (p >0.05). On the other hand, patients with Type II were more likely to have two screws (31.25%) than Type I (12.5%) and Type III (18.75%; p =0.042).
The association between the number of screws and other parameters are listed in Table 7. The distribution of the number of screws was not significantly associated with age (p =0.513), gender (p =0.169), laterality (p =0.33), and most of the medical comorbidities (p >0.05). On the other hand, patients with two screws had significantly higher BMI (31.4 vs 25Kg/m2 in patients with one screw; p =0.019). While the preoperative IMA was lower in patients with two screws (13.5 vs 20.65 patients with one screw; p =0.011). Patients with one screw were more likely to have hypertension and osteopenia (p =0.012 each).
Discussion
Metatarsal explosion is a new complication in bunion surgery that did not exist until the new modernization of minimally invasive techniques. The combination of unorthodox metatarsal realignment, refined screw fixation/orientation and bone resection create a biomechanical scenario for specific fracture failure patterns. While the term, metatarsal explosion might seem dramatic, it’s an accurate representation of the extreme comminution and positional displacements that occur specific to these new minimally invasive methods. This investigation not only classifies these fractures, but provides an understanding of the mechanism and treatment paradigm for this inevitable bunion surgery complication.
While complications are unavoidable with bunion surgery, new MIBS has an overall reported complication rate of 0 to 42%.15–19 Specifically, regarding metatarsal fractures after MIBS, other surgeons have documented their presence, however these injuries have not been specifically studied or classified in totality.15,20–22 Gordon and colleagues, in their landmark MIBS study of 292 cases identified 6 patients who had “screw-bone interface failure” at the distal lateral first metatarsal cortex, they label as “metatarsal cut-out” and are seemingly equivalent to our Type I metatarsal explosion.23 Frigg et al experienced one case of fracture dislocation in 48 cases, which required reoperation with no further details given.24
We identified a pattern and mechanism for the three types of metatarsal explosions as well as three variables that dictate the type of metatarsal explosion. The variables are: 1) location where the primary MI bone screw (a term we coin the “anchor screw”) exited the lateral metatarsal shaft, in other words the proximity of the anchor screw’s exit to the osteotomy, 2) the direction the fracture line progressed (distal or proximal), and 3) stability of the anchor screw’s head within the metatarsal base (a term we coin, “anchoring”). A second MI screw (we term the collateral screw) was identified as present and the above variables also pertain to this additional point of fixation.
The mechanism for fracture failures all seemed to have originated where the anchor screw penetrated/exited the lateral metatarsal cortex in the CPZ. The “cortical real estate” (another term we coin) is the amount of cortical bone surrounding the anchor screw at this exit point, determined whether a fracture would initially extend distally or proximally. Little cortical real estate, in other words, a shallow cortical rim between the anchor screw exit point and osteotomy resulted in a fracture line that only migrates distally into the osteotomy, creating the Type I metatarsal explosion. When there is greater cortical real estate between the osteotomy and the anchor screw, then the fracture can propagate both distally and proximally, splitting the metatarsal shaft transversely. Fractures that also extend proximally throughout the bone are segregated based on the trajectory of the fracture line. Those that extend intra-articularly into the first tarsometatarsal joint, while avoiding the head of the anchor screw, are classified as the Type II metatarsal explosion. Fractures that split the first metatarsal directly along the plane of the anchor screw are classified as the Type III metatarsal explosion.
The stability and location of the head of the anchor screw within the metatarsal base appear to be important factors in determining the pathway of fracture, and if a fracture pattern will be stable or unstable. It appears the stronger the head of the anchor screw is anchored into the cancellous bone, the less likely the fracture will dislodge the head. Instead, the fracture extends plantar to the anchor screw into the first metatarsal cuneiform joint. An anchor screw’s head that is positioned in the dorsal aspect of the metatarsal base results in an obliquely oriented screw that seems to be more susceptible to destabilization from retrograde ground reactive forces with weightbearing. Similarly, when the anchor screw is not placed within the medial cancellous bone of the metatarsal base, aka the CAZ, but rather placed further distal in the medial cortex of the bone also appears to have a propensity to equally destabilize the cortex through stress risers, particularly if a collateral screw is used.
The majority and most common metatarsal explosions were Type I (occurring at the distal lateral metatarsal cortex between the screw and the osteotomy) involving (8 feet), accounting for half of all metatarsal explosions. The other half of metatarsal explosions occurred proximally, with Type II accounting for 31% (5 feet) and Type III accounting for 19% (3 feet). Type III metatarsal explosions were the least common.
Anchor screw placement and positioning of the entry point in the CAZ and exit point within the CPZ plays a role in the development and pattern (type) of metatarsal explosion. A distally placed screw in the CPZ was present in 75% of all metatarsal explosions, and 87.5% of Type I metatarsal explosions. This emphasizes how important it is to maintain cortical stability within the CPZ with increased cortical real estate, which can be achieved by exiting the cortex as proximal on the lateral metatarsal as feasible or achievable. A distal and/or dorsally anchored screw in the CAZ was present in 50% of Type II & III metatarsal explosions. This suggests that anchoring the screw’s head within the cancellous bone of the metatarsal by avoiding dorsal and distal placement might help prevent or limit proximal fracture propagation. It also suggests that obliquely placed screws, or those not centrally positioned in the sagittal plane of the first metatarsal, may contribute to a load pattern that results in bone failure. A combined CPZ and CAZ issue was seen in 20% of Type I and 50% of the combined Type II & III metatarsal explosions, also pointing to the need to carefully consider both the anchor screw’s entry and exit points within the first metatarsal. Fixation that addresses the structural anatomic constraints of the first metatarsal might be better suited to resist or limit metatarsal explosion.
Management of metatarsal explosion is on a case-by-case basis with a deep understanding of the patient’s medical comorbidities, psychological state, expectations, social situation, and severity of the metatarsal explosion should be considered. An argument could be made for surgically correcting any metatarsal explosion, regardless of type, as the position is changed from that of the initial surgery. However, any attempted surgical repair after new MIBS is complicated by bone loss from the index surgery and fragmentation of new fracture(s) with or without comminution.
.jpeg)
.jpeg)
The majority of metatarsal explosions (12 feet, 75%) were treated non-operatively with protected partial weight bearing in either a CAM boot or postop shoe. Surgery involving open reduction internal fixation was generally reserved for the more violent fractures (Type II & Type III). Type I metatarsal explosions generally maintain an ‘acceptable’ overall position, despite the loss of fixation stability. These were treated conservatively in 7 of the 8 feet (Figure 5). Type II metatarsal explosions also were mostly treated without surgery in 5 feet (31.25%), despite being a violent injury with a disturbing appearing radiograph (Figure 6). Type III metatarsal explosions are unstable and underwent surgery in 2 of 3 feet (Figure 7). When the head of the screw is adequately anchored and positioned in the CAZ, it might provide a protective effect in preventing fracture propagation but we are speculating and an area for biomechanical studies.
.jpeg)
It is important to recognize that metatarsal explosion is multifactorial involving patient factors (i.e., medical comorbidities – such as diabetes, thyroid and/or osteopenia, BMI), postoperative weight bearing, surgeon technique, fixation construct and device design. Independently and/or collectively these factors may contribute to the development of a metatarsal explosion. Patient selection for health and adherence to a ‘reasonable’ postoperative weight bearing protocol should be considered. Best practices that aid surgeons to deliver reproducible consistent anchor screw placement would be beneficial tools no matter the level of surgeon experience. Lastly, implants that are designed to combat these variables that lead to fracture failure might help lessen these complications.
This was a retrospective study that critically evaluated a new complication with new MIBS that has not been previous studied or fully reported. While this is the first study of its kind, we expect that other surgeons will now report in detail on this complication. Perhaps other types of metatarsal explosions will arise, adding to this new classification we developed. We make assumptions on possible etiologies and variables that contribute to metatarsal explosion, but having screws distal within the CPZ and/or distal/dorsal in the CAZ may not lead to metatarsal explosion on a case-by-case basis.
Conclusion
In conclusion, new minimally invasive bunion surgery with percutaneous screw fixation has given rise to a new complication we term metatarsal explosion. We classified the three types of metatarsal explosion, proposed etiologic cause and a mechanism of occurrence. Two screw fixation of MIBS was more likely to have a metatarsal fracture. Metatarsal explosion is an uncommon complication, though we believe inevitable, in a bunion surgery practice adopting this new bunion surgery. This manuscript should serve as an aid to best practices that will help improve outcomes, lessen metatarsal explosion, and provide a basis for treatment/management.
Disclosure Statement
Neal M. Blitz DPM is the CEO of Voom Medical Devices, Inc and receives compensation for this role. David T. Wong DPM reported no disclosures. Eric S. Baskin DPM is the Director of Surgeon Training for Voom Medical Devices, Inc and receives compensation for this role.
Financial Declaration
The authors received no financial support for the research, authorship, and/or publication of this article. Artistic drawings/renders provided by Voom Medical Devices, Inc.
Funding
None
Author Contributions
All authors have reviewed the final manuscript prior to submission. All the authors have contributed significantly to the manuscript, per the International Committee of Medical Journal Editors criteria of authorship.
Acknowledgments
Bogdan Grecea DPM
Kenny Luong DPM
Corresponding Author
Neal M. Blitz, DPM
Email: nealblitz@gmail.com